РЕЛИГИЯ И ПСИХИЧЕСКОЕ ЗДОРОВЬЕ
Aннотация
В этой статье мы представим эмпирическое исследование, мотивированное желанием изучить влияние религии на психическое здоровье через сравнение ответов респондентов из числа сербского населения в целом, из числа приверженцев господствующей религии и небольших конфессиональных общин, а также психиатрических пациентов. Выборка состоит из 621 респондента: верующих Сербской Православной Церкви, Адвентистов Седьмого Дня, баптистов, и пятидесятников (N=303); населения в целом (N=225) и пациентов психиатрических клиник (N=94). Использовалась программа обработки данных MMPI-201. Вопросы, на которые пытается ответить данная статья, следующие: на какие переменные, связанные с психическим здоровьем, влияют религии, и приводит ли религия к улучшению или к угрозе психическому здоровью? Каким образом общество устанавливает критерии для оценки «другого» и «отличающегося», и как это отражается на самооценке подростков? Эти и ряд других вопросов, поставленных в процессе работы, открывают возможность практического применения данного исследования.Ключевые слова: религиозность, психическое здоровье, депрессия, православные, адвентисты, пятидесятники, баптисты
К сожалению, текст статьи доступен только на Английском
Introduction
The importance of religion is steadily increasing. This is recognized in different ways, but primarily in a number of religious buildings in our immediate surroundings – both in places where they were torn down and in places where they have never existed before. Confessional religious education has been included in the curriculum of public schools and children (in some places it is obligatory, while in other they can choose to have religious education) are exposed to religious influences much more than it was previously the case. There are more friends of ours who celebrate Slavas again, and this may be true for us, too. Some new, young people look for religious values, visit churches and religious communities. Some go to monasteries, others join new religious movements, or become inspired by religions of other cultures (Smith and Faris, 2002; Kuburić and Moe, 2006; Kuburić and Kuburić-Borović, 2009; Kuburić and Zuković, 2010; Kuburić and Gavrilović, 2012; Blagojević, 2013; Kuburić, 2014).
Searching for the purpose, many come to religion as a system that stands firmly on its foundation set either in the religion revealed long ago, or in a long-established tradition. Whatever the case may be, the process of secularization, which threatened previous generations with forgetting the religion, has shifted its direction towards the process of desecularization or revitalization of religion. Sociologists search for new theories of religion, for the old ones, based on Marx’s criticism of religion as the opium of the people, have lost their significance. Psychotherapists are not entirely sure according to which value system they are to assess religious problematics in their attempts to answer the needs of individuals, families and the transitional society (Šušnjić, 1998, Hamilton, 2003; Kecmanović, 2001).
At the same time, we hear (less than we used to hear before), at least when Serbia is in focus, the media mentioning sects, pointing out danger that threatens individuals and their families. Religious tensions build up between large religious traditions – Christianity and Islam. In such a trend of increasingly mistrusting the religiously Other, we hear calls for tolerance and becoming familiar with others with the aim of living together in a pluralistic society, which cannot be avoided any more (Moe, 2009; Kuburić, 2010; Kuburić, 2013).
What is religion in the context of individual religiosity?
Religion is a very complex phenomenon, most frequently analyzed and observed through the prism of its teachings, which are more or less adopted in the course of socialization in the family, church, and the society in general. However, William James (1990) believed that theories born out of religion were multifarious and therefore secondary. The state of believing may contain just a minimum of intellect. The essence of a religious experience lies in feelings and behavior. Therefore, the cognition that brings an individual into the area of the sacred is based on the faith, which is a highly individual phenomenon. A measure of individual religiosity is a personal experience of a believer with his or her God, reflected on his or her life. A religious institution is an organized form of a religious life, which concretizes into religious communities and interpersonal relations in a given time and place.
Does a life of an individual, and particularly does one’s mental health, depend on a concrete religious teaching? Are there better and worse religious organizations, and which of them beneficially affects mental health? In order to obtain correct answers, hypothesizing is certainly not enough. Empirical researches have the purpose to eliminate a doubt, while defining terms allows clear communication and mutual understanding.
In attempt to define religion back in 1912, J. Leuba cited 48 definitions of religion in his «Psychological Study of Religion» and added several definitions of his own (Gill, 1969). Since that time, different authors have given their contribution by their own varied definitions of religion. For instance, Đuro Šušnjić (1998) says that everyone knows in one’s own way what religion is, but here, terminological knowledge is required. Although he is against definition, he believes that it is better to have some definition than none at the beginning of a study, but one should not take it too seriously. He offers an overview of different definitions, tests them and criticizes, and finally he establishes his own definition which does not contain a value judgment. Every «belief in absolute and mystic power» can be regarded as religion, for this belief is an important and common characteristic of all religions (Šušnjić, 1998:81). Religion is a special life-style, which is described in its teaching, expressed in its symbols, reflected in its highest values, prescribed in its norms, realized in communities of believers, toughened by its institutions, embodied in its holy persons, felt in holy places and in holy times (Šušnjić, 1998:50).
Religiosity appears as an individual aspect of religious phenomenon, which can be defined as a subjective system of attitudes and as a system of inner, permanent dispositions, which include beliefs, knowledge, feelings and behaviors. Religiosity is occupation of man with an idea that God exists. Belief in a being more powerful than man is a starting impulse of forming a world view that explains all important questions. It is a system of knowledge about God and men, about the past and the future, life, death and salvation, woven into religious teachings, which is transmitted from generation to generation, yet understood and interpreted anew. Religious feelings, depending on a type of adopted religion, can be positive, negative and fluctuating, depending on the feeling of guilt and responsibility before God, as well as on the feeling of love and gratitude. Religiosity pervades a person and it is observable in behavior of believers in religious rites and rituals, as well as in everyday life style (Kuburić, 1997; Kuburić, 1999).
Religious thinking is qualitatively different in different phases of personality development. There are phases of religiosity of children and religiosity of adults. From infantile to mature religiosity, personal development unfolds due to a synergy of many factors. One can talk about normal developmental phases, which occur with age and maturation, but also about phases of religiosity, which are independent of age, but depend on religious experience (Kuburić, 2013).
It is common for all religions that they consist of two parts: discomfort, that is, a feeling that something is wrong with us in our natural state; and salvation, a feeling that we are saved from misapprehensions by establishing a proper contact with higher powers. If an individual suffers for his or her misapprehensions and judges them, then he or she has already consciously overcome them. An example of such an experience can be found in the Book of Isaiah, when he saw God’s glory and said: «Woe is me! for I am undone; because I am a man of unclean lips, and I dwell in the midst of a people of unclean lips: for mine eyes have seen the King, the Lord of hosts[1]« (Isa. 6:5). The encounter with God results in a consciousness about oneself as well as in discomfort. In the case of the prophet Isaiah, the salvation comes from God: «And he laid it upon my mouth, and said, Lo, this hath touched thy lips; and thine iniquity is taken away, and thy sin purged.» (Isa. 6:7).
In the second developmental phase, a man identifies himself with a better part of him and becomes aware that this higher part of his is similar and connected to God, in whose likeness it was created. That closeness to the divine being causes safety and joy, which, as an acquired mood, refreshes vital forces, gives strength to endure, fills up with passion and meaning, as well as with magic or majesty. The goal of religion, in the final analysis, is life, more encompassing, richer, more satisfying; love toward living is a religious drive, which connects man with the source of life.
Already with this knowledge, an assumption is clearly stated that religion has a powerful impact on a personality, by means of bringing it down to the bottom of anthropological disappointment, on one hand, and bringing it to the euphoria of internal divine being, on the other. It appears that religion makes it possible to learn limits of human possibilities, as well as how to overcome those limits. In any case, religious experience has a profound effect on a personality, and its effects are not insignificant for mental health.
Defining a personality, like defining religion, is a very difficult and almost impossible task. Already in 1937, Gordon Allport analyzed by that time gathered definitions of personality (there were already 48) and came to a conclusion that all authors were right in some way and that it was not possible to bring all these different definitions down to a common denominator. «An individual, whatever else it may be, is one internal, consequent and unique organization of bodily and mental processes» (Allport, 1969:18). Although Allport alone expressed pessimism concerning the possibility to terminologically determine personality, most studies of personality accept his definition (Hrnjica, 1994), which states: «Personality is a dynamic organization, inside the person, of psychophysical systems that create the person's characteristic patterns of behavior, thoughts, and feelings» (Allport, 1969: 44).
Personality, which functions as a whole in interaction with everything that exists around it, is difficult to be explained by its parts and process. Namely, there are two realities – an internal and an external one. Life is interlacing, weaving, touching of the inner and outer worlds, each time in a new and unrepeatable way. The product of this meeting is an experience which we can name personality. It realizes itself by living, on the foundation of a genetic play. A wealth of genetic potential and laws of functions have been enabled and determined probably by God Himself, who cannot be, naturally, either defined or understood, but only assume as a Personality of the Universe, celestial intelligence, absolute truth and integrative power of everything that exists.
Understanding a healthy personality has also varied in contests of time and space. How can limits of sanity be determined in this variety of individualities? Each personality is different, but an ill personality differs from others by failure to fit its difference into a harmonious unity of the system called the life in a community with oneself and significant others. The question is not whether religiosity in itself is healthy or pathological, but how to distinguish between healthy and pathological religiosity. Religion in its history has offended individuals, and the main method of misuse is found in fear, which religion has intensified, instead of reducing it (Delumeau, 1986).
Amfilohije, the Metropolitan of Montenegro and the Littoral (1994) defined religiosity as a pursuit of salvation from meaninglessness. It is a longing for a vertical, which gives meaning and balance to the horizontal of existence, and, in essence, all this is a pursuit of health. He believes that not every religiosity is healthy (that is why the effects of religiosity on human life and behavior are not always the same), because there are two kinds of religiosity. Healthy religiosity allows realization of the very human nature and gives knowledge of what man is and what part in man gives the true meaning, and how this meaning is realized. Contrary to this modest religiosity, which gives joy to life, there is magical religiosity, which possesses a longing for the completeness of being, for the root, health, knowing the truth of all things; however, its reaches, postulates, and ways of satisfying this longing, instead of bringing to its goal, lead away from it, frequently eclipsing the life itself and helping the disease. The reason for it lies probably in understanding God. Magic wants, without much effort, to reach its goal, knowledge and health of soul and body. Its relation toward the divine is mechanical and utilitarian. It encourages either blind and suicidal sacrifice or mechanical manipulation with God; it nurtures blind fear and nefarious arrogance. An important difference between healthy and false religiosity lies in that the former builds its safety on trust, which makes it healthy. «The Nature is healthy, always good, given to men for good and prosperity – that is what the human nature is like. Each human being is a joy and wealth of all existing worlds. No being is without purpose, dignity and a role in worlds. If so, then there is no reason for any human being to feel insignificant and worthless. There is no being without a gift, which distinguishes them from other beings and completes other beings; if there is nothing else, then the gift is their very existence» (Amfilohije, 1994: 17).
Are healthy religiosity and healthy personality in correlation?
An extensive work on religion and health, published in 2001 on more than 700 pages (Koenig, McCullough and Larson, 2001), represents a significant achievement in the history of medicine, because, for the first time, a critical overview and review of empirical studies were given in one place, supporting the effect of religious involvement. The book predominantly analyzed western religious traditions. The analysis of results of over 1,200 studies and 400 researches during the twentieth century, showed both positive and negative «effects» of religion on health during life from the childhood and the adolescence to the maturity and the old age. Chapters on mental health and religion (Koenig, McCullough and Larson, 2001: 97-228) cite the following positive effects: feelings of wellbeing, happiness and satisfaction with life, hope and optimism, meaning of life, higher self-esteem, more social support and less loneliness, lower incidence rate of depression and faster recovery from it, lower rate of suicide, less anxiety, less psychotic tendencies, abuse of alcohol and drugs, delinquent and criminal behavior and higher marital stability and satisfaction. As a negative effect, it is mentioned that excessive commitment to religious practices or religious social activities reflects in negligence of the loved ones and family life. A person dedicated to religion, either through prayer and studying or religious activities, may neglect his wife, children and other obligations of life, including also his job. Dedication to church and voluntary activities instead of meeting needs of the family members results in an unhappy family life, which increases stress for all family members. Furthermore, a rigid interpretation of religious scriptures, such as taking out of context and approving violence, leads to mental and physical abuse of the spouse and children.
Gary Collins (1988: 117) in his book «Christian Counseling» cites Durkheim’s conclusion (Durkheim S. 1887, Suicide reprint, Glencoe, III.: Free Press, 1951) that religious people are less prone to suicide than the irreligious. According to Durkheim, this is because religion integrates people into a group. Less lonely and isolated, these people are less prone to depression and attempts of suicide. Churches and other social institutions can become therapeutic communities, where people feel welcome and accepted. Other researches also show that religion is an important factor which determines a subjective feeling of satisfaction with life (Kecmanović, 2001). People who regularly attend church feel happier than those who don’t (Allen, 1990: 123). A nationwide study on the young and religion (Smith and Faris, 2002) showed that the religious young had more positive attitudes toward the life than their less religious counterparts. Regular church or religious community attendance and active belonging are correlated with higher self-esteem and positive self-image.
Jovan Marić (1995) wrote that the following factors affect the evaluation of the suicide risk: a stress situation, recent divorce, rejection, job loss and love loss. Nevertheless, patients who have obligations to their families and who seriously take care of their obligations have lower risk than persons who do not feel themselves obligated to help others. However, the risk increases when a person begins to think than he harms the close ones and that he is a burden to them. The question how religion affects suicidal behavior can be indirectly answered by indicating religious teachings on the value and the holiness of life. The Sixth Commandment of the Decalogue is: «Thou shalt not kill» (Exod. 20:13). If we remember Christ’s commandment to love oneself and the neighbor: «Thou shalt love thy neighbor as thyself» (Matt 22:39), we can understand that its function is to protect life. Basically, religious teachings are aimed at controlling aggressive and sexual urges. Religious teachings, but also attending church provides a social support and has a healthy impact on life. Religious and socially active people have a significant advantage over those who are isolated or who lack in faith.
A research on a sample of believers and the general population conducted in Serbia (Kuburić, 1995; 2008; Kuburić, 2014) showed a relation between variables of mental health – psychopathology and other self-image variables, family variables and variables of religiosity. Based on results, we discovered that mental health had a high correlation with variables of psychological self, above all emotional maturity, positive body image, impulse control and adaptability. Social and family relations are very important for mental health, as well as all family variables, save religious education. The coefficient of correlation (0.17) between trust in God and mental health indicate a weak connection between these variables. However, more attention should be paid to the variable of «way of Salvation», which is the only religious variable that has a significant correlation with psychopathology variable (p=0.34). To be specific, believing in God’s unconditional love and justification by faith has a positive correlation with mental health. The conclusion is that there is no connection between religious affiliation of parents and mental health of children. Frequent religious rituals within a family are not directly connected with mental health of children. However, they can indirectly contribute in a way that allows children grow up into healthy personalities if, during these family celebrations, they develop trust in God and His love, instead of fear and the feeling of guilt, if that contributes to cognitive understanding of the world and the life, and if they do not create too big a gap between what is real – possible and ideal.
From the mentioned researches and experts’ opinions, we can conclude that religiosity and active involvement in religious life contribute to mental health, but that exaggeration leads to the opposite. However, maintaining mental health is not a characteristic of believers alone, and social support is not a characteristic only of religious communities. For that reason, we want to focus our attention in this paper onto a comparative analysis of different social groups.
Which variables in the system of mental health are influenced by religion, does religion make it stronger or jeopardize it? In what way religion determines criteria for evaluating the Other and the different and how does it reflect on a self-image? These and many other questions asked in this paper open up a possibility for a practical application of the results of this research.
EMPIRICAL RESEACH
Subject and aim of the research
The subject of this study is the analysis of relations between religiosity and mental health of believers of the Orthodox and Protestant Churches in relation to the general population and the population of psychiatric patients in Serbia. The main aim of the research is to examine effects that religiosity has on mental health and to check whether there are differences between different types of religiosity and religious affiliation (churches and sects).
A conceptual framework of the research contained several groups of research objectives. The first objective was to determine whether there were differences between adherents of confessional communities (this is what the non-traditional communities are called in the 2006 Law) and members of smaller religious communities (which are commonly called sects in Serbia). For that purpose, we compared results obtained from member of the Christian Adventist Church with those of members of the Pentecostal and Baptist Church. The second objective was to determine whether there were differences between members of the confessional communities and members of the dominant religious community, i.e. the Serbian Orthodox Church. In order to fulfill this objective, we compared results obtained from Orthodox theology students with those obtained from Protestant theology students in Belgrade. The third objective of this research was to check whether there were differences between believers and the general population. This objective was achieved by comparing theology students with students from the general population. We started from an assumption that the strongest religious identity is seen in those who decided to live on and by religion. The objective was to compare students of Orthodox and Protestant theology – Christians in different ways – with the general population of students.
In this research, we started from the null hypothesis, an assumption that there are no statistically significant differences between the observed religious groups. The objectives mentioned above were the first three hypotheses, and in order to evaluate the test itself (which is designed for diagnostic use in psychology) and the forth hypothesis (related to statistically significant differences between psychiatric patients and general population), we compared results of the patients with the rest of the sample.
Method
The research was conducted according to concepts of cross-sectional studies, in which comparative method is used. Respondents were tested, which allowed us to process data quantitatively. Furthermore, general information on respondents and their statements on the role of religion in their life were also collected. The statements on religion made a quantitative analysis also possible, which helps us to better understand spirituality of different types of church organizations.
The situation of testing was nonselective. Everyone present, either at church, school or hospital, could take the test on a voluntary basis – if they wanted to do so. Respondents were told that the testing was for academic research purposes and that everyone, who wanted, could be informed on their own psychologically interpreted results in an individual conversation. All respondents were given a telephone number which they could call and they were encouraged to use this opportunity (this was used by one third of the respondents).
Instruments of the research and variables
The dependent variables in this research are MMPI-201 scales. Factors that are considered to be the independent variables are all those that directly or indirectly can contribute to differences on the dependent variables: gender, age, marital status, profession, financial status, number of family members, whether they live in a complete or an incomplete family, religious adherence to a church, a sect or an atheist, christening – whether a person was christened or not (and if yes, whether they were christened as children or as adults), for how long they have been believers, how they came to accept their faith – in their families or they, on their own, accepted a teaching different from a teaching their families hold to.
The Minnesota Multiphasic Personality Inventory (MMPI), created in 1940 (published for the first time in 1943) is, in its design, a multidimensional personality inventory, containing 566 items, which can be generally grouped into 26 topics: from general health, neurological problems, through marital and family problems, to political, sexual and professional affinities (Lemke and Wiersma, 1976; Biro and Berger, 1981; Berger, 1984).
The original scale with 566 items is rarely used in practice. Results show that the item stability and reliability of the entire questionnaire drop sharply after approximately 180 items, indicating that average human ability to withstand the «test effort» lies somewhere around this number (Biro and Berger, 1981: 38). For that reason, modifications are needed, as well as shortening. This will remain a challenge for young researchers to make new modifications. Mikloš Biro and Josip Berger made a short and modified version – MMPI-201, which is the test used in this research (Biro and Berger, 1981; Biro and Berger, 1986).
The test is very reliable as an indicator of reactions to stress. Our first idea, at the beginning of this research, was to examine whether believers are more resistant to stress than the general secular population. In clinical practice, the test is used in diagnostics, for selecting patients and evaluation of the course and effects of the therapeutic treatment. Each person is an individual concreteness, a personality with its own developmental capacities, experiences and behavior. It is difficult to generalize and set borders between what is healthy and what is disordered, and to infer, in scientific endeavor, about general phenomena. These are limitations and challenges this research is facing.
The MMPI is an instrument based on self-evaluation and the principle of measuring dimension. The instrument is neutral when it comes to understanding the very nature of madness – is it a disorder (like a failure in the organism due to physical-chemical or biological disorder) or a conflict (a result of a conflict within an individual between biological and social needs, when one or another force overpowers the other, due to slackening of mental structure and processes), or deviation (like an atypical lifestyle or «unconstructive individualism») (Biro and Berger, 1981). Nevertheless, the MMPI best depicts a deviation that is, as a lifestyle, in opposition to the family, society and culture.
The MMPI is designed to detect pathology. Concerning psychiatric disorders, it is possible to consider both qualitative and quantitative differences between normality and psychopathology. Depending on our starting concept, we can research into psychopathology as a deviation from the normality. Distribution of raw scores and their relation with T-scores (a T-score of 50 is an arithmetic mean, and T-scores of 70 and 30 are two SDs (standard deviations) away from AM (arithmetic mean). It is possible to consider the existence of qualitative differences between the normality and psychopathology, that is, to consider categorial instead of dimensional distribution of psychiatric disorders. The test has 11 scales, three of which are control scales – also called validity scales and their purpose is to check suitability and readiness of respondents for this kind of a test, i.e. a degree of confidence we may have in obtained results. These are the L-scale, F-scale, and K-scale.
The L-scale or the Lie scale is a variant of a questionnaire that was used also in earlier research into moral behavior. Within this questionnaire, it is used to assess the level of temptation to falsify answers by choosing always those that put a respondent in a socially acceptable light. It can be also used as an indicator of some specific personality characteristics – rigidity, naivety… (Biro and Berger, 1986). Namely, according to Berger (1984: 338) the highest score on this scale will be achieved by someone who is perfectly sinless, that it a saint, a prude, a flawless hero and, naturally, a liar. However, there is a limit, empirically set by a score; if this limit is overstepped, the test is marked or invalidated. A very high score indicates that a moralizing protective behavior is so strong and far-reaching that the MMPI cannot make a reliable profile of pathological (negative) tendencies. Some authors recommend the upper limit at the T-score of 70. For this research, the L-scale is very important, maybe even crucial, because of the very link between religiosity and morality – a need to respond to God’s holiness with human sinlessness. In religious persons, two tendencies are present: some, like the Pharisee, hide their sinfulness behind public religiosity; yet others, out of their sinfulness, dare not lift up their head before God (Luke 18:10-13). Religious hubris – hypocrisy is as much present in believers as the feeling of sinfulness. This scale helps us recognize these two tendencies.
The F-scale is a scale of strange answers or atypical behavior. A high score on this scale can have different backgrounds. The most common case of increasing the F-score is seen in inattentive respondents: they answer «blindly», without reading the questions, without understanding them (because of the lack of literacy or education). There is also a tendency to simulate, or a tendency to think in a confused way and give bizarre answers, which is often found in psychoses. A high F causes an increase in scores in most other scales, and it lies in correlation with clinical scales.
The K-scale or scale of the feeling of power (superiority or inferiority) is seen as a reflection of suppression, i.e. defense against the expansion of pathology. Some patients systematically exaggerate when they present their condition, while others show the opposite behavior and diminish the severity of their disorder. In this game of addition and subtraction while describing oneself, the task of this scale is to correct the bias. Contrary to the L-scale, the source of high scores on the K-scale is usually in the area of subconsciousness. A high K-score indicates a good control, as well as preserved defense mechanism, while a low score on this scale indicates a need of a respondent to express his pathology, i.e. a tendency to self-criticism, but also a conscious «forcing» a pathological self-image (if the F-score is also high). Most authors recommend the T-score of 70 as an upper limit of tolerance for this scale.
In this research we find very important just two scales. The D-scale measures the depth of clinically conditioned complex of symptoms, which constitute a depressive syndrome. A high D may indicate the only or the main pathological formation of a respondent, but it is usually an element that accompanies other psychopathological characteristics, such as characteristics of low emotional energy, along with the feeling of uselessness and inability to accept normal optimism regarding the future. A person who reacts to frustration with depression lacks in self-confidence, he or she is introverted and is constantly worried for someone or about something (Biro and Berger, 1986). Depressive characteristics that are especially accentuated are: despondency, decrease in emotional and life energy, low level of intentionality and spontaneity, tendency to self-accusation, feeling of the lack of prospect, helplessness and worthlessness. Anxiety is easily noticed and it manifests itself in many different ways (also in a somatic form). Persons of this type are perfectionists and pedantic. Symptoms that indicate a disorder of vital functions, such as libido, appetite and sleep, are commonly seen. A hereditary tendency to this kind of reactions has been proven (Biro and Berger, 1981). They are caring parents and souses, hardworking, critical of others but also of themselves. They have a compulsory need to maintain order. Although they are deeply committed to their job and they accept responsibilities, this excessive commitment tires them out quickly and increases the feeling of insufficiency.
The Ma-scale relates to a hyperactive, extrovert, sociable personality. With quick associations and euphoric mood, this person frequently is in the center of attention, and their cheerfulness and humor arouse sympathies. These persons tend to overestimate their abilities and take many projects and simultaneous activities. There are also present hypervigilance, increased sexual activity and internal restlessness. A hyperactive person is cheerful and undertakes many tasks with great enthusiasm, but is usually not able to finish them. Problems: psychomotor agitation, inability to concentrate, talkativeness, exaggerated motoric and gesticulation. Some questions in this scale are merely emphasizing normal answers, which frequently increase a score of normal respondents. This profile is found in extremely extroverted personalities, people who show great enterprise, and those who tend to «pull» their surrounding and colleagues in any kind of activity.
Impressions from the testing
Comments of believers regarding the MMPI-201 and certain questions in it can help us to better understand both our respondents and the test itself. Right at the very beginning, believers indicated that there was a difference in their lifestyles before and after conversion. Naturally, those who had experienced conversion asked if they were to write about their «old» or «new» life. Other comments related to whom they were to compare themselves to while assessing. One level is a human-human relation, and the other level of understanding the test is when one looks at the relation between man and God.
Applied statistical procedures
«In order to objectively study the main source of variances in the MMPI, most researches used factor analysis. Results were mixed and they depended on whether the factor analysis is conducted on the level of items or the level of a scale, as well as on the specificity of the sample» (Biro and Berger, 1981:46).
After the testing, the data were codified, entered into tables and processed using the SPSS program. Statistical processing of the data served the main goal – to determine differences between the groups of respondents. The simplest case of differentiating between respondents is when differences between the arithmetic means of two groups of respondents are analyzed in relation to one manifest or latent variable. As the first and clear insight and a possibility of graphic presentation of the results, arithmetic means and standard deviations for all groups were calculated. Significant difference on variables of the MMPI-201 test was also calculated. Variance analysis confirmed all present differences in a multidimensional space of the researched variables. For calculating relationships between variables, the linear correlation coefficient was used. Since the subject of this research is multivariant, it was needed to determine a smaller number of basic variables, which explain such a mutual correlation, so we used factor analysis, or more precisely, principle component method. Canonical discriminant analysis as used as a method for multivariant data analysis. This allowed us to determine the maximum separation line between the researched groups, as well as real structures of their differences, i.e. latent content dimensions which separate them.
Sample
The total number of respondents in this research was 621. It was formed from different groups, which are relevant for this study. The target group was a group of believers of the Protestant churches who make up to a half of the sample. The second segment of the study was concerned with student of the public university (Faculty of Philosophy, Faculty of Electrical Engineering, Faculty of Agriculture, in total N=134) and students of theology (Orthodox theology at the Faculty of Theology in Belgrade N=80 and Protestant theology in Belgrade N=88; in total N=302 students).
Characteristics of the sample
During this research, 621 respondents were studied, of whom 312 (50.2%) were males and 309 (48.8%) females. Most of the respondents filled out the tests at their university or church – 527 (85%), but in order to compare different groups using the instrument with clinical scales, we tested 94 psychiatric patients as well. They, like students from the general populations, were not asked about their religious affiliation.
According to self-evaluation, 127 (20.5%) were atheists, while 494 (79.5%) were believers. It was common for their family members to belong to the same religion, so the majority of the respondents share the religion with their parents (62.8%). However, 37.2% stated that they were alone in their faith, either because their parents were atheists or because they accepted a Protestant type of religiosity. These proportions are not related to the general population in Serbia, but only to a sample with respondents sorted out into groups of almost equal number of respondents. This is because our aim was not to examine the sociological structure of the population, but psychological effects that religiosity exerts on mental health of believers. The proportion of the Protestants in the general population is approximately 1% (Kuburić, 1997).
The sample in this research is consisted of almost equal number of five different population groups (general population – students of secular faculties; believers – theology students of Orthodox and Protestant theology; patients of psychiatric institutions). Since the selection of respondents was not conducted, the sample simultaneously represents a social structure of the examined groups. So, in the sample of believers, females are much more numerous, as well as they look for a help in psychiatric institutions in a larger number. However, the situation at the faculties of theology is completely opposite. There are twice as many young men who study theology than young women. In this way the balance in gender structure is achieved in the total sample.
On the sample of our respondents, we may test an assumption that stress and accumulated life experience cause women to react neurotically, passively or with a withdrawal and sickness, while men react actively, and if aggression is too high, their reactions are destructive and psychopathic. Perhaps we can recognize here the nature of women’s «hidden sexuality» (Toševski, 1994) and the nature of the female being in general, as well. A suppressed energy, forbidden to manifest itself, is directed toward the inside of a female being, where it grows and develops. If she does not succeed in creativity, beauty, giving birth and love, woman reacts with an internal suffering, which destroys her more than others, producing a need for salvation. For that reason, Christian churches are full of women who seek God’s mercy.
Although women are more numerous in Christian churches, they are more dissatisfied with their churches than men (Kuburić, 1996). Whether this is a result of emotional instability, great expectations or truly poor behavior of men toward women within the institution of marriage and church, it is a question yet to be answered by researchers.
Table 1
Number of family members in the total sample is as follows:
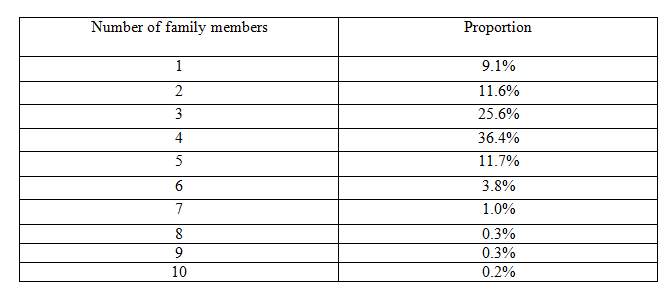
420 respondent live in a complete family (68.6%), while 201 (32.4%) live without one of the parents.
Most of respondents believe they live averagely, like other people they know – 446 (75%). Above the average, in good financial standing, there are 87 (14%), while 68 (11%) respondents live below the average financial status.
Characteristics of the subsample of psychiatric patients N=94
More than a half of psychiatric patients who sought psychological help at the Institute for Neuropsychological Disorders «Laza Lazarević» during 1998 and filled out the MMPI-201 questionnaire were between 18 and 28 years of age. If we observe the distribution by gender, we can notice that men and women are different in that men seek psychological help at the age of 18. The number steadily decreases toward the age of 28. The forties are again a period of crisis, when a number of men come back or seek psychiatric help. Among women, 18, 23, 28, 40s, and 50s are the most common ages found in the population of psychiatric patients. Furthermore, the number of women who seek psychiatric help is larger than the number of men, which is the case in other studies as well (Kuburić, 2009).
In our sample of psychiatric patients, there are 61.3% of women and 38.7% of men. 28% of patients live in marriage, while 72% have no spouse. Those who live in a complete family make up 61.3% of the sample, and 38.7% live in an incomplete family. The distribution of number of family members with whom these patients live is as follows: 4 (35%), 3 (24%), 2 (14%), 1 (13%), 5 (8%), 6 (2%), 7 (2%) and 8 and more (1%). Regarding diagnosis, depressive characteristics are dominant in the population of psychiatric patients.
RESULTS OF THE RESEARCH
Interrelation of psychological dimensions from the intercorrelation matrix indicates a large number of statistically significant, high and moderately high correlations. From that large number of variables, it was needed to set a smaller number of basic variables or factors which explain such a mutual relation, which was done by factor analysis, i.e. principle component analysis. Out of 11 independent variables, factor analysis singled out three principle components or three factors, which explain 76% of the common variance of the whole system.
Table 2
Characteristic roots and explained parts of manifested variance variables
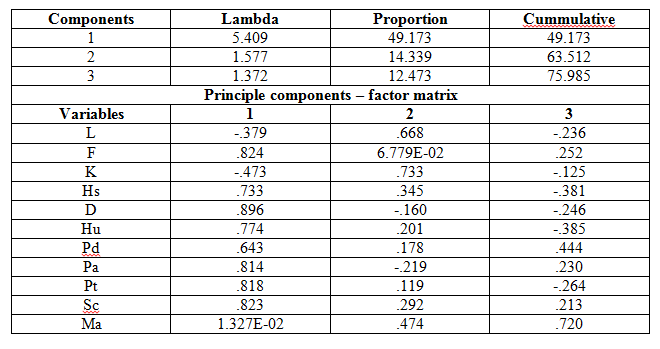
Isolating characteristic values of the most important latent variables was done by the Guttman-Kaiser criterion. Based on the obtained results, factor analysis brings us to the conclusion that the first component is generally psychopathology that manifests itself through self-accusation, self-pity and passive-aggressive behavior. The first factor which explains 49% of the total variance, and includes almost all clinical scales, with very high saturation of 0.896 for the depression scale, then F (0.824); Sc (0.823); Pt (0,818); Pa (0,814); Hu (0,774); Hs (0,733) and the lowest saturation for Pd (0,643).
The second principle component (factor 2) is the most saturated variable which determines the approach to the test, representing oneself (which has two tendencies: a tendency to hide pathology and a tendency to openly show the presence of symptoms that means seeking help). This factor saturates the L scale (0.668) and the K-scale (0.733).
The third principle component is most saturated with the Ma-scale (0.720), which represents stress activity, emotional maturity or immaturity, and hyperactivity.
Therefore, based on the factor analysis of the dependent variables in this research, we can conclude that the variables are grouped into three important factors: clinical picture, approach to the test and readiness to use mental energy in a constructive way.
Differences between believers, general population, and psychiatric patients
The aim of this part of the research was to determine whether there are statistically significant differences across respondents from the general population, believers, and psychiatric patients in the system of the observed variables. If statistically significant differences exist, we want to determine which variables contribute most to those differences between the samples of respondents. In order to realize the set goal, canonical discriminant analysis was used for data processing.
Psychiatric patients in relation to the general population
We believe the first thing that has to be brought up concerning the results are differences between healthy and ill respondents, or, better to say, those who were tested at universities and those tested at churches and psychiatric hospitals. The MMPI test was designed for diagnostic purposes, so our position about the results will be the best if we compare MMPI-201 results of the patients with the results of the respondents from the general population and then to look for a place of the believers in our research, who express their religiosity either by studying theology or by belonging to a small religious community which they frequently attend (at least once a week) and who are ready to display their religious identity, which is not especially valued by the society.
The discriminant analysis isolated only one discriminant function that is statistically significant for discriminating groups of respondents in the examined discriminant space.
Table 3
Discriminant analysis for the general population and psychiatric patients
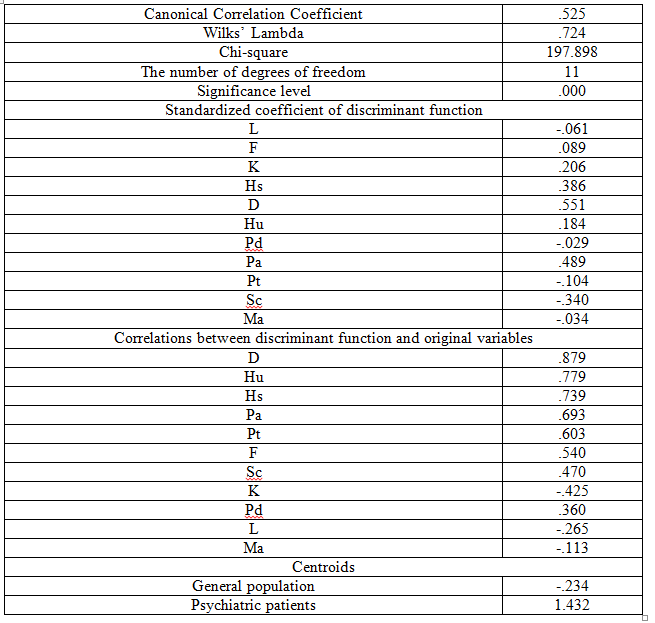
Table 4
Arithmetic means (M) and Standard deviations (SD) on the variables of the MMPI-201 test for the sample of general population (N=527) and the sample of psychiatric patients (N=94)
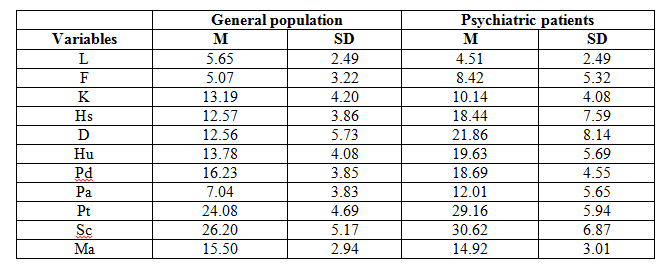
If we draw a profile according to the presented results, it can be well seen that they perfectly fit into the T-score of 50 for our sample of the general population, which insignificant increase on the Pd and Ma scales, which can be interpreted to show that religiosity, which dominates in our sample, is against conformism, majority and submissiveness. Arithmetic means of psychiatric patients are slightly below the T score of 70, which indicates that psychopathology is two standard deviations away from the distribution of the general population. A drop is only present in the Ma-score, where our two distributions meet. There are more extroverted individuals in our sample, who are more inclined to activities and enterprise. Namely, Christians are really inclined to «pull» their close ones on the way of salvation. In the sample of psychiatric patients, depressive elements are dominant and decreased mental energy is also noticeable.
Differences between theology students and students of secular faculties
The aim of this part of the research was to determine whether there are statistically significant differences between the respondents of the general population and theology students within the system of the observed variables. If statistically significant differences exist, we want to determine which variables contribute most to those differences between the samples of respondents. In order to realize the set goal, canonical discriminant analysis was used for data processing.
The discriminant analysis isolated only one discriminant function that is statistically significant for discriminating groups of respondents in the examined discriminant space.
Table 5
Discriminant analysis for theologians and secular students
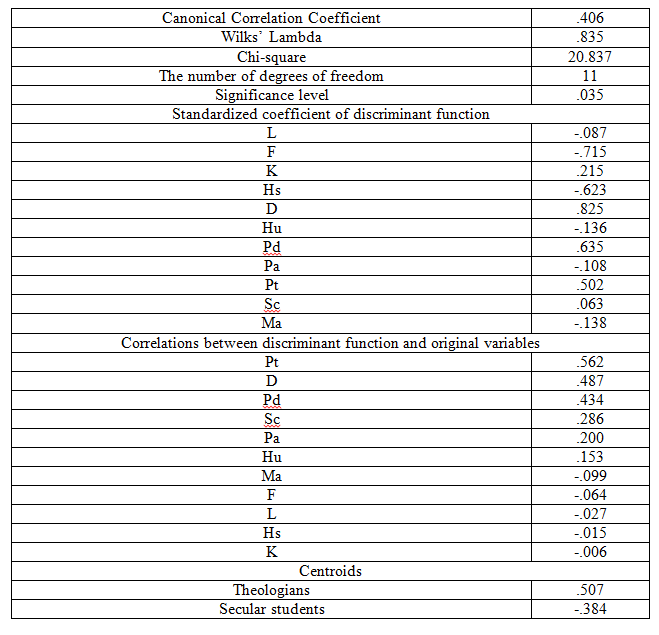
Theology students have a higher score on the control scales, which indicates a possible unwillingness to expose their own negative characteristics as well as a certain level of rigidity. From the religious aspect, flexibility, compromises and indulging a sin are not positive characteristics, so this can be viewed as a quality of religiosity. An accentuated need not to commit a sin is characteristic for believers, which is close to perfectionism; but sensitivity to already committed sin is also typical, when, under the influence of conscience, they make their lives bearable by suppression.
A difference on the Pd-scale is significant on a level of 0.01 indicating a higher level of disrespect for human authority among the religious. If these results are compared with the results of previous studies (Kuburić and Kuburić, 2006), according to which, morality and empathy are stronger among religious persons, then we can interpret this by saying that in circumstances of secular society, when religion was unpopular, religiosity was a characteristics of people inclined to individualism, so disrespect for social norms relates to accepting religion as a personal value system, which can be further understood as a decreased ability of social adjustment.
In the Church, as an institution, there are many rules of behavior, especially among Adventists, and they represent increased behavior surveillance. In that way, already present empathy in correlation with moral behavior is enhanced by the context of law and surveillance in a religious community. Heteronomous morality, which can be labeled as a religious legalism, is suitable as a framework that protects believers from experimenting with social adjustment and creates rigid personalities in service of safety. Keeping away from «sins», which almost always occur in interpersonal relations, causes social isolation, which can be complete – monkhood, or group isolation – different smaller religious communities, sects, cults, which become self-sufficient in their quest for salvation (Vernette, 1997; Kolarić, 1987; Đorđević, 1990, Hill, 1987).
For the sample of theology students, we can say that they are efficient, productive and active, which is indicated by an increase on the Ma-scale, for which it is known that it has a tendency of increasing in so called normal profiles (insisting on one’s own health and normality), and on the other hand, it depicts members of this sample as extroverted, enterprising and ambitious personalities.
Differences between students of Orthodox and Protestant theology
Table 6
Arithmetic means and standard deviations on variables of the MMPI-201 for students of the Orthodox (N=80) and Protestant (N=88) theology
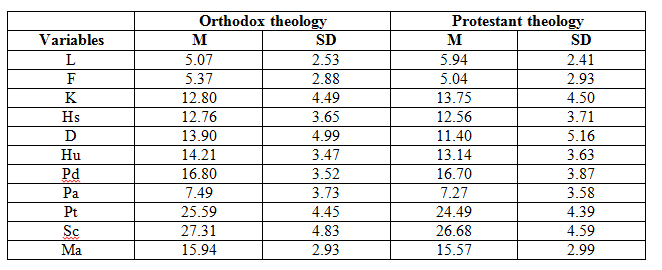
Variance analysis for students of the Orthodox and Protestant theology shows that the only differences exists on the L (0.05) and D (0.01) variables, which indicates an increase on the L-scale of the Protestant theology students and higher level of depression among the Orthodox theology students. An increased need to hide themselves and to give a better picture of themselves can be caused by increased neuroticism or, simply, by morality. Both characteristics were found in previous researches (Kuburić, 2013).
Discussion of the study results
Interpretations of the MMPI went from analyzing individual scales, through combining the most prominent scales, to sequential a typological approach. Profile analysis, based on interrelation of certain scales and on the two (or rather three) the most increased scales, shows that most widely used principle of MMPI interpretation demand an excellent clinical experience (Biro and Berger, 1981). In this research, we did not deal with individual profiles and their analysis, but with groups of respondents and their mutual differences. Statistically significant differences, on same scale, indicate tendencies that are present in a group that we compare.
Certain items in the questionnaire can help us to better understand differences between religious and irreligious respondents. For instance, item: «I know precisely who is responsible for most of my problems». As believers understand it, this usually refers to the tempter of humans and the enemy of God. Several times during the testing, a question was asked whether these claims referred to humans only. Namely, an idea that someone attempts to influence someone else’s life, thoughts and behavior can refer to God or to His enemy. A believer is aware of the importance of these beings in his own life and he gives them greater significance than to influences by other humans. Believing in God makes a person, on one hand, more open minded and allows a different understanding of the reality. We cannot interpret everything religious as pathological. Like any other thing in life, religiosity can be healthy, but it can also be disordered, depending on a person and his ability to put the faith in the service of a healthy lifestyle or else faith can become a factor that drags him away from a healthy lifestyle. A difference between a vision and hallucination was beautifully described by Vladeta Jerotić (1997).
An importance of limits that religion imposes was discussed by a believer who noticed: «When I doubted the law, everything in my life collapsed.» Safety is based on rules given by God Almighty. Wanting to help other people to rise from their chaos, this believer tries to find a scientific proof for God’s existence. His idea is that there should be an effort on a cognitive acquisition of knowledge about God, so that these convictions can affect emotional safety. Namely, when a person believes in God, a step that follows is getting to know God, who he is and what he is like in a relation to man. Necessarily, there is a fear because of one’s own sinfulness and unworthiness. What does God ask and expect? Directing oneself according to God’s demands is the way of morality. Here, a question of the psychological state of a person who has had a religious experience. The question is: What is an optimal level of religiosity, which allows maturation of a person up to an autonomous morality, without psychopathological consequences?
There is a type of religiosity that is directed to self-accusation and annihilation of joy in life and enthusiasm that leads to activity and joy of completion, as if it supports psychopathology. Withdrawing from life, a wish not to give birth, desire to disappear, and passivity are more destructive than constructive behaviors, against life, against activity, against sexuality, against commitment. In a religious experience, withdrawing in one’s own individuality, with no communication with the outside world, can represent the utmost form of religiosity, which is completion and joy of meeting powerful personalities in faith. However, a correct interpretation always lies in context of the life of a person and his surroundings.
Christian believers have a tendency to live an active life, which wins other people. Missionary activities, music, prayer, everything is in the service of wining people for the eternal life. To approach another person is not a rude behavior, but an imperative of wining souls for Christ. Due to the feeling of transience of life and importance of saving people, a level of functioning rises, not because of some internal need that is rooted in pathology of a person, but because of the mission that engages all potentials.
According to a study of Jelena Vlajković (1998), for more successful and less risky course of a crisis, a great importance lies in a social support, which a person in a crisis gets from his social surroundings. An internal locus of control and looking at the future are also connected with a successful course of a crisis. Almost all religions offer a community of believers, which has a possibility, like an extended family, to provide a social support to a fallow believer. A function of integrating believers, through common beliefs and participation in ceremonies, provides safety and protection, offers a hope for the future that overcomes boundaries of the worldly life. That is the reason why they spontaneously feel that it is possible to find peace and the purpose of life in church; especially adolescents, when they feel internal turmoil as a result of growing up and taking up roles of adults. They gladly join religious communities which offer them a stabile value system and limits that give safety.
Conclusion
Based to the results of the research, we learn that differences between healthy and ill respondents are significant on all variables, while differences between groups of believers are slightly present only on some variables. Based on factor analysis of the dependent variables in this research, three important factors were isolated: clinical scales, approach to the test and readiness to use mental energy in a constructive way. According to the results of discriminant analysis, the starting hypotheses are confirm, that is, there are no statistically significant differences between members of the Orthodox and Protestant churches in Serbia on the clinical scales. Furthermore, the difference regarding mental health between believer and the general population is not significant. There are differences on the scales that measure the approach to testing and willingness to speak openly about oneself, but also on the third factor, which represents readiness to constructively use mental energy.
In interpretation of the results, an advantage is given to the idea that religious respondents organize their psychological functioning by relying on religious teachings, which shape a value system and moral behavior. For orthodox believers, who belong to a religious community of a traditional type, religious rituals and community is important, because they provide a feeling of safety and belonging. Religious norms are also an important support for mental health, since they give safety and a backing in mental functioning and recognizing limits.
Religion as a rationalization of suffering and the Church as a therapeutic community allow catharsis through rites along with cognitive mechanism of understanding the Salvation. Facing their own fear and uncertainty of life, questioning the meaning of life and astonished by the wealth of unrealized possibilities, which vanish in the blink of an eye, intelligent, both in a cognitive and in an emotional way, young people seek a system that is powerful enough to provide them safety and to reduce anxiety. Like psychology, theology also offers a possibility of better understating of oneself, through cognition, as well as the possibility of actively helping others. The value system of the institution based on traditional values and organized according to a tested model, which integrates all aspects of knowledge and activity, from religious teaching to ritualistic and mystic experience.
The meaning of life offered by religion is one of its main functions. Viktor Frankl (1981; 1982; 1985), in his logotherapy, recognizes the role of religion in treating mental disorders. Vladeta Jerotić (1997) wrote that Christian individualistic way is not a way that leads to a blissful state without conflicts, fear, or doubts; this way is not any kind of celestial harmony on the Earth without feeling of guilt and without guilt. However, this way is a designed way, where every new fear and a new guilt are experienced as a call from God to greater perfection toward «the measure and completeness of Christ».
However, that first phase in religion, which causes a feeling of guilt in believers, is in the service of choosing orientation and direction, improving oneself and one’s own personality, working toward the salvation from sin. In the process of conversion, in meeting with God, man feels himself tiny. That painful feeling motivates man to seek a help from God, to seek forgiveness and salvation, which every theology understands in its own way. In Christianity, the rituals of christening and feet washing symbolically remove the guilt from a man and bring back self-esteem, which is accepted by association with the clean and the powerful, symbolized by a white dress. Justification by faith is a powerful instrument in theology, which has psychotherapeutic effects.
The Orthodox theology, according to the results of this research, appears to nurture some kind of sorrow. The feeling of guilt, present in consciousness of believers, indicates a life permeated with suffering. Saints were usually martyrs, who came to enlightenment through suffering. Suffering, as a cathartic experience, is sometimes wished for, and one lives with it. However, in Protestant theology, there is a need of avoiding suffering, it is symbolically experienced in rituals, and one frees oneself from it through work, order, and responsibility, in other words, through an organized lifestyle, which is achieved by internalization of religious norms in the process of individualization.
Christian hope is based on withstanding evil and actively pointing to good. Naturally, this is more theory than practice. However, on a level of psychological functioning, we can notice that Christian believers have accentuated personality characteristic such as sharpened conscience and lower threshold of feeling guilt. At the same time, there is self-overestimation; believers think they are more moral than others are. There is also hostility manifested as a self-accusation and higher discontent with one’s own body, whose aggressive and sexual urges are recognized. Torn between «I can» and «I want», which is a situation expressed in words of Paul the Apostle: «O wretched man that I am! who shall deliver me from the body of this death? … for to will is present with me; but how to perform that which is good I find not.» (Romans 7:24, 7:18)
Salvation – faith and/or deeds, orientation toward God’s example, crucified and resurrected Christ give a possibility of seeking one’s own balance and measure in religious life. Exaggerating in any direction is a symptom of psychopathology. A paradox lies there, that only then, when man surrenders himself to the salvation by faith and gives up on good deeds, good deeds became a factor of salvation, because there is no place for a reword in morality. Christianity has for two millennia provided satisfaction of spiritual needs of man and has given a measure of developing a personality, which goes from building up faith in oneself, other fellow human, and God, to self-realization in the individualization process that allows autonomous morality and responsibility toward life. Christian perfectionism inspires optimism, but it also permits depression, which is connected with the lack of understating, disappointment, or failure in Christian life.
[1] Translator’s note: The King James Version is used for all quotations from the Bible, since it is the closest to the Serbian translation of the Bible used by the authors.










Список литературы